Spasticity can significantly impact quality of life in people with neurological injuries and disorders by disturbing gross motor patterns (i.e. gait, grip). Spasticity is usually treated with medication and/or orthosis. Classical understanding of spasticity was that it cannot be reduced once it becomes a chronic problem.
Spastic muscle activation can be objectively visualized with electromyography (EMG), identified by the inability of antagonistic muscles to coordinate forces at a single joint. An example of this is “foot drag” during the swing phase of a gait pattern — while gastrosoleus complex is supposed to be relatively relaxed, spasticity in these muscles plantarflexes the ankle, causing the foot to drag.
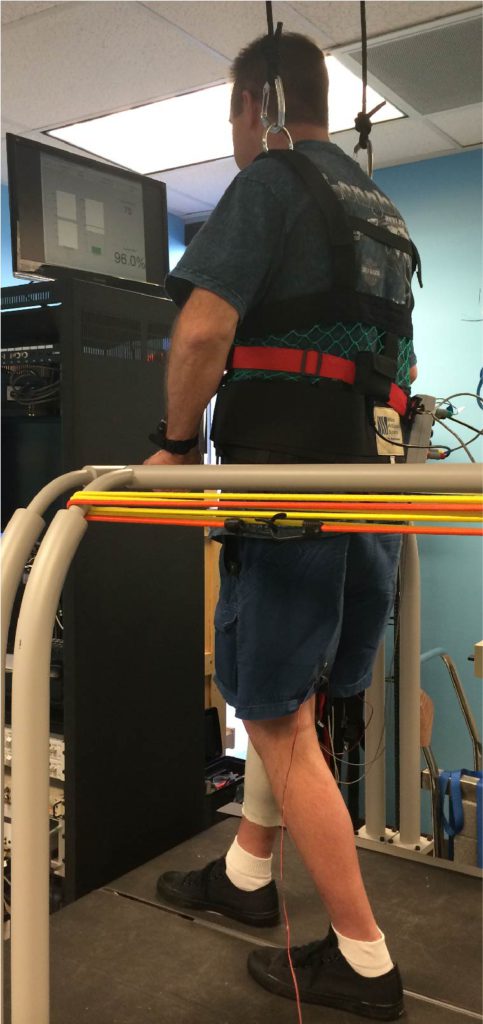
Operant Conditioning for spasticity is performed by providing electrical stimulation through a peripheral nerve. The size of the Hoffmann (H) -reflex is measured. Its size is controlled throughout a movement in adults with no known neurological deficits, however people with spasticity has uncontrolled spinal excitation shown as large H-reflex size on EMG.
Effects On Gait
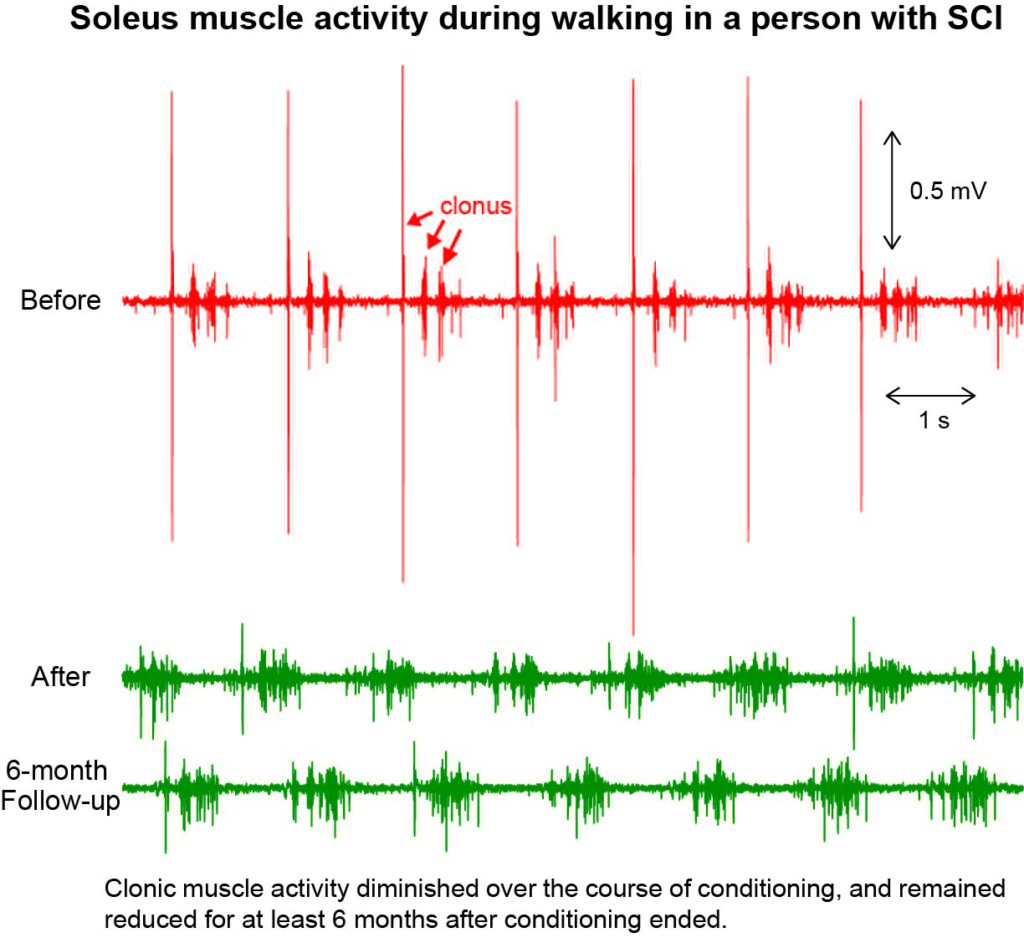
Successful down-conditioning of reflex can decrease spasticity as shown below. The image shows multiple clonic EMG profile of soleus during the terminal stance through swing phase of gait in a person with incomplete spinal cord injury. Clonus in soleus causes involuntary dorsiflexion, which is usually treated with medication and/or orthosis. After down-conditioning the soleus reflex while weight-bearing through both legs, this person was able to show changes in EMG activity while walking. Soleus is now shown to be silent during swing phase of gait.